This post is about how I realized I have ADHD, what my symptoms were, and how I managed it with Bupropion.
Let me prefix this by saying that none of this is medical advice: I’m just an autistic software engineer with a lot of free time. If you have mental health problems, for the love of God just talk to a psychiatrist. I promise it’s not bad. Psychiatry is good, antidepressants aren’t happy pills that zombify you, and the pharmaceutical industry has saved countless lives. That aside, let’s begin.
An Epiphany
I have a funny story of how I realized I have ADHD.
In late 2017 I started taking fluvoxamine for anxiety. It helped, but partially, so the psychiatrist added aripiprazole, an atypical antipsychotic sometimes used as an adjuvant to SSRIs.
I had to quit after a week because of Parkinsonian tremors (it turns out that fluvoxamine inhibits the cytochrome that metabolizes aripiprazole, so I was effectively getting a higher dose). But that was the most productive week I’d had in ages. After years of burnout, I had the mental energy and motivation to do things. I resumed work on my personal projects. I stopped procrastinating. I was studying things that interest me. I felt like the person I am.
I told this to three psychiatrists but none of them seemed to think it was meaningful. One of them offered to restart me on aripiprazole, but I didn’t want to risk tardive dyskinesia. So I went back to being a lazy bum.
Years later, while going down an autistic special interest rabbithole, I got interested in pharmacology. I bought a copy of Molecular Neuropharmacology. And I didn’t read it (because I didn’t have the executive function) but I did leaf through it. And in the first chapter I read about how partial agonists work.
Briefly: low dopamine activity makes you ADHD, high dopamine activity makes you schizophrenic. That’s why stimulants (which increase dopamine) can cause psychosis. A partial agonist of dopamine acts as an agonist (dopamine ↑) when dopamine is low, but acts as an antagonist (dopamine ↓) when dopamine is high. In short: partial agonists are stabilizers. Aripiprazole is a partial agonist of dopamine.
And I had an epiphany. And I looked it up: can Aripiprazole be used to treat ADHD? I found a case report report of a woman with ADHD who was treated with aripiprazole, she reported exactly what I experienced, down to the daytime sleepiness. I found a clinical trial where aripiprazole was successfully used for ADHD.
This was 2022. It took me four years to figure it out (it turns out it’s hard to solve problems when you keep getting distracted from them), but who can say they’ve diagnosed themselves from first principles after an unusual reaction to a drug?
And I talked about it with friends who have ADHD, and things began falling into place.
Symptoms
For someone who has 500 tabs of PubMed open at all times it’s embarrassing how long it took me to put things together. I think, partly, it’s because life-long pathologies are hard to notice: we know mental states by mutual contrast, if you’ve never been very focused or effective you might not think of yourself as a particularly unfocused or unproductive person.
Partly, also, because everything in the DSM overlaps: someone who is anhedonic and has low executive function could be ADHD, or they could also be chronically depressed, or even schizophrenic1. Chronic decision paralysis is an aspect of ADHD, but also of anxiety. And so on.
Partly because whenever I’d try to tell a psychiatrist about my horrible problems with finishing projects they’d redirect to some other topic they felt was more important.
And partly it’s because we make physical and mental deficiencies into moral ones. I’ve spent vastly more time castigating myself for being undisciplined, lazy, etc. than I’ve spent rationally and systematically trying to solve my problems.
But everyone who has undergone successful psychiatric treatment understands: we are automata, like the gears of Babbage; we travel in fixed orbits, as predictable as the orbits of the planets, and the movements of objects in space.
So a lot of these things only became visible as symptoms of ADHD after the fact, after discussing it with friends who have ADHD and with my psychiatrist:
-
Autism: obviously I have ASD (I told the psychiatrist who diagnosed me it would be more surprising if I didn’t) and ADHD co-occurs “in 30–80% of individuals with ASD”.
-
Focus: I never felt like I was particularly distractible or unfocused, mostly because I’ve unwittingly structured me life around not having to focus, using various coping skills, mostly centered around text.
I’ve always struggled with paying attention during meetings, but I just thought that’s because the meetings were pointless. I was very surprised when, after initiating Bupropion, I suddenly realized during a work meeting that I’d been paying attention for multiple minutes on end without having to remember to take notes.
I’ve tried meditation time and time again but I felt unable to make progress with it, because I’d lose focus within seconds. When I looked for advice on how to overcome this, people online would say: “just observe your thoughts”. But the whole problem is that the thoughts surface on their own, and carry me away before I can notice them, and it’s frustrating to resume meditating when you realize you’ve spent the past five minutes writing code in your head.
-
Physical Restlessness: my default mode of thinking is to pace the room endlessly, which I’d chalked up to autistic stimming2. When seated I’ll drum my feet, if my legs are crossed I’ll often shake the foot that’s off the ground.
-
Low Self-Control: for years on end, every day I’d tell myself, “today we’re going to sleep at a reasonable hour”. The alarm would go off, and I’d find some excuse—I have to finish this Wikipedia rabbithole, or finish this video, or read one more paper—to stay up, and go to sleep somewhere between 1 and 5 am. This was a big problem. Unfortunately the Bupropion doesn’t exactly help here because the twice-daily dosing schedule gives me a bit of insomnia.
Wikipedia in particular is like a time machine. I go to the front page, intending to look something up, click on the featured article—and come to forty five minutes later with twenty open tabs, somehow having gone from “Enceladus” to “List of Allied bombings raids on Wilhelmshaven in World War II”. My life is like Memento: I wake up with no recollection of who I am but instead of tattoos I have all these PDFs I’ll never read.
-
Productivity: Austral took years to finish. Years. So much so that at a certain point I became embarrassed to bring it up, because I knew that when I did, people thought, “oh, yeah, that’s Fernando’s idée fixe that he keeps saying he’ll finish”. It took so long because I’d start working on it, and run out of steam, and leave it untouched for months and months on end. The commit log reflects this: tall, narrow peaks of hyperfocus separated by long stretches of inactivity.
The Epiphany of Gliese 581 is barely a novella at 26k words. It took me a year to finish. I worked on it by accumulating fragments that came to me spontaneously, then growing text around them like geological strata, until the fragments began to touch in time. And it shows, in the structure: the frequent
<hr>breaks are simply where I joined too fragments without connecting tissue. The idea of sitting down and writing it down, linearly, chapter by chapter and paragraph by paragraph was beyond ridiculous. I could hardly sit down to get three paragraphs out of my head at a time.Sometimes I’d get a burst of executive function, and I’d be able to work on a project consistently for a weekend or even a week or two. And I’d rack my brain to figure out: what did I do differently, and how do I extend this? Is it my diet? Have I accidentally fixed some persistent nutritional deficiency? Is it my caffeine dosing schedule? Should I do 150mg of caffeine in the morning and a cup of tea in the afternoon? What’s the clearance rate of sugar-free Monster? Maybe I can supplement L-tyrosine since it’s a dopamine precursor. I’d try to twist every knob: caffeine intake, sun exposure, cardio, lifting, micronutrients, etc. And nothing worked consistently.
It made it extremely difficult to plan for the future, because I had no idea when or how long I could work on something.
-
Chronic Underachievement: I start an ambitious project, and it withers away. I dropped out of college. I start reading a book, put it away and forget it. The years pass, the projects remain unfinished. What I have achieved was achieved by white knuckling through it, at the cost of persistent burnout. This is a great source of pain, because I’m a creative person, and it hurts if I can’t create.
-
Engineering Methodology: I suppose this is somewhat self-serving, but the north star of all of my engineering work is complexity. I always insist on simplifying, keeping moving parts to a minimum, ensuring the whole system is small enough that it fits in my head so I can reason about it.
I designed Austral to be a programming language that I would enjoy using. Now I realize that the entire language is designed as an assistive technology for a programmer with ADHD.
The core language principle is simplicity. Everything is as explicit as possible, and implicit behaviour (like type conversions and exception propagation) are thrown out: this helps because everything you need to reason about the code is right there on the page. It places minimal demands on working memory. Writing code is, effectively, about serializing your working memory, and reading code is about restoring that serialization. If I get distracted, it doesn’t matter, because I can just read the code again to restore context.
There is a whole list of anti-features, things I threw away explicitly to reduce cognitive overhead. The linear type system is designed to be based on a small core set of simple rules that fit on a page. The module system, with the separation of module interfaces and bodies, is designed to minimize how much I have to read and hold in working memory in order to work. The language’s features are designed to be overwhelmingly orthogonal. I threw out async because async + linear types is hard to reason about. I threw out exceptions because exceptions are hard to reason about.
What Didn’t Work
I resent when people say to stop taking pills because the solution to [insert mental health] problem is exercise. First, because I can outlift everyone who tells me that, and secondly because I feel that it confuses cause and effect. If someone has crippling depression, and they start a rigorous exercise routine, that might just mean they’ve spontaneously entered remission. So if your anxiety or whatever can be handled by exercise and drinking a mango smoothie: good for you. Please don’t tell me about it.
Here’s the things that didn’t help with my ADHD: todo lists, the X effect, Vipassana meditation, lifting, cardio, methylated vitamin B12, vitamin D, magnesium, zinc, keto, carnivore, vegetarian, generic talk therapy. More generally: pharmacology is the only thing that’s even changed anything for me, and the “classical” or non-pharmacological approaches only become useful with pharmacological assistance.
It was only after I started taking Bupropion that I was able to use a todo list consistently, that I was able to make spaced repetition into a daily habit, that I was able to build up productive habits and practices.
My mental model of this is: when your reward function is just $f(x) = 0$, putting effort on a productive task gives you as much reward as putting no effort at all, or procrastinating on some instant-gratification Skinner box. Habit formation becomes impossible. You might manage to use a todo list consistently for a week, or two weeks, but eventually something happens that breaks that streak, and you find that despite repeated effort, you have not formed a habit. The associations in your brain simply are not there.
Bupropion
Bupropion, also known as Wellbutrin, is an antidepressant. And an aid in quitting smoking. And a treatment for ADHD.
Chemically, it’s a substituted amphetamine; in terms of its activity on receptors it’s an NDRI, a norepinephrine-dopamine reuptake inhibitor. It binds to NET and DAT, effectively increasing the activity of norepinephine and dopamine. And for this reason, it has a stimulant effect.
The reason it’s classed as an antidepressant rather than a stimulant is the stimulant effect is very mild (which is why actual stimulants are the first choice in ADHD treatment) and it’s not a euphoriant. People rarely try to abuse it, with horrible results, but it’s more likely to kill you than get you high.
There are three formulations:
- Immediate release (IR)
- Sustained release (SR)
- Extended release (XR or XL)
SR is typically two 150mg pills taken eight hours apart, XL is usually one 300mg pill taken once daily. SR is safer than IR and XL is safer than SR, because the more extended the release, the lower the peak concentration, and the effects of Bupropion are proportional to its plasma concentration.
I suppose most doctors would prescribe the XL by default for this reason. In Australia, however, SR is the only version available3, so I had to take 300mg twice daily. This isn’t great more sleep (more on this later) but 300mg is more effective than 150mg.
Effects
Since starting Bupropion I’ve observed the following positive changes:
-
Anxiety: it didn’t eliminate anxiety, but it did reduce it by about 20%. This is surprising, since for some people Bupropion has the opposite effect and makes them more anxious.
-
Intrusive Thoughts: these were vastly reduced, along with negative self-talk.
-
Low Mood: before starting Bupropion, I occasionally had days where I was in a very low mood. Since starting Bupropion, I’ve not had what I would call a bad day, where I feel terrible and just want to stay in bed. This is distinct from anxiety, which I still struggle with despite the Bupropion: I still have moments of blindingly acute anxiety, but not low mood or depression. Overall most of the time I feel optimistic.
-
Productivity: Bupropion increased my productivity by about 10%-30%. The effect is fairly muted: I don’t feel more energetic, but empirically I can look at my output and see that it has increased. Occasionally, I am able to dedicate an entire day to hyperfocusing on a problem, most of the time, the benefit is I can simply start something and do a few hours of work.
Bupropion gave me enough executive function to overcome the worst of ADHD and to allow me to “bootstrap” productivity. Since starting Bupropion, I:
- Started using a todo list daily and effectively.
- Became able to consciously form good habits, including doing spaced repetition daily.
- Became much better at keeping on top of chores, including keeping the apartment clean.
So it’s not superhuman productivity, but I can make progress on projects and stay on top of chores. Doing creative work no longer feels like I’m in a hostage negotiation with my own brain.
There are still things I procrastinate on. Correspondence is something I struggle a lot with, I’m ashamed to think of all the emails in my archive where people have reached out to me and I procrastinated on replying to them until it became too embarrassing to even reply apologetically. But I now have the tools to at least improve things.
Interestingly the effects were not immediate, but gradual, since doubling to 300mg daily I felt like productivity increasing like a gentle ramp-up across weeks and even months. It was like unlocking skills in a video game: I first unlocked the todo list, then the calendar, then the Pomodoro timer, etc.
-
Anhedonia: before Bupropion, I could easily experience negative emotion (mostly anxiety) but positive emotion was very muted. My emotional range topped out at “content”. Formerly pleasurable activities such as reading, playing videogames, watching movies brought me little to now joy. With Bupropion I can enjoy things a bit more (even though all movies are bad).
-
Accomplishments: after years of on-and-off work, I managed to finish Austral4. After a year of struggling to put a single paragraph down on the page, I finished The Epiphany of Gliese 581. It was still difficult, still time consuming, but I had enough help to manage. The work paid off. I felt that I succeeded: my reward function was non-zero.
There’s other empirical evidence that my productivity increased. For example: this blog. I asked GPT-4 to write a script to make a histogram of posts per year for this blog:
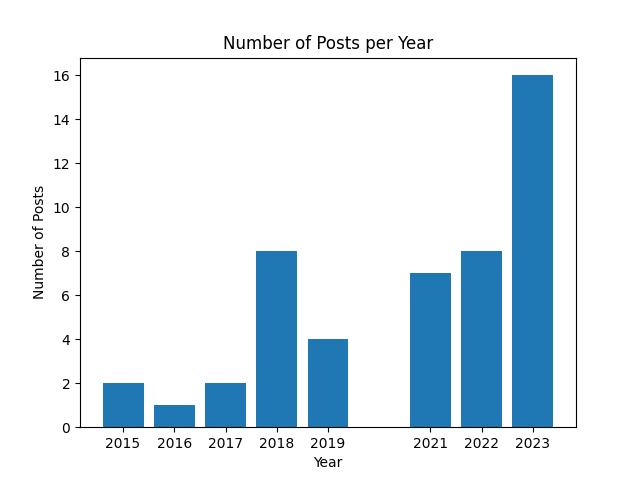
2020 was a bad year. Note (if you’re from the future) that 2023 covers only Q1.
Side Effects
Some side effects I experienced:
- Rash: this appears to be a common problem, judging from r/Bupropion search results. Within two weeks of taking Bupropion, I felt itchy and saw the skin around my neck was erythematous. It didn’t feel life threatening but it did look consistent with an allergic reaction. So, acting on medical advice, I discontinued Bupropion, took desloratadine for a month, and then tried starting the Bupropion again. The rash didn’t come back, so it couldn’t have been an allergic reaction.
- Appetite: the first day I took it I forgot to eat until I almost went to bed. This went away within a few days. Bupropion is a known anorectic.
- Insomnia: this was strongest the first few days I took it (150mg once daily) and quickly subsided. But when I moved to taking it twice daily the insomnia became more of a problem. Because the spacing between the doses is so long (8h), I’d often forget to take the second dose on time, so I’d take it later, which means I’d go to sleep later, wake up later, take the next first dose later, and so it’s a vicious cycle of sleep schedule drift.
There are known side effects which I did not experience but merit a mention:
- Seizure: the headlining risk of Bupropion is seizures. Bupropion lowers the seizure threshold, if you have a history of seizures, this is worth mentioning to the doctor. My read on this is that, early on, Bupropion was prescribed in much higher doses (500 or 600mg or higher) and in immediate release formulations, which led to many instances of seizures. Nowadays dosage stops at 400mg/day, and is typically just 300mg/day, and overwhelmingly in the form of sustained release or extended release formulations, which have lower peak concentrations. So modern formulations and doses are much safer. More on this below.
- Worsening Depression: some people report that Bupropion worsens their mood. I know at least two people who reported it made them feel more depressed.
- Psychosis: I don’t know the incidence but, as with stimulants, sometimes this happens.
- Alcohol: this is a known bad interaction with Bupropion since it further lowers the seizure threshold. I just avoided drinking.
See Also
- Bupropion on MedlinePlus. Searching anything medical on Google turns up nothing but spam, I like MedlinePlus because it’s accurate and there’s no SEO bullshit.
- Robert Wiblin’s account about his experience with Bupropion.
- Scott Alexander’s practice website has a page on Bupropion.
- Zimmerman et. al. 2005, Why isn’t bupropion the most frequently prescribed antidepressant?.
- Stahl et. al. 2004, A Review of the Neuropharmacology of Bupropion, a Dual Norepinephrine and Dopamine Reuptake Inhibitor.
Appendix: Data on Seizure Risk
From 15 Years of Clinical Experience With Bupropion HCl: From Bupropion to Bupropion SR to Bupropion XL by Fava et. al., 2005:
An important adverse event associated with bupropion use is seizure. With the IR formulation, the rate is 0.4% (4/1000) at doses of 300 to 450 mg/day; however, the rate increases substantially at doses above this level. With the SR formulation, the rate is 0.1% (1/1000) at the target dose of 300 mg/day. The incidence of seizure with bupropion XL has not been evaluated. Bupropion is not the only antidepressant associated with seizures. SSRI antidepressants are associated with seizure at a similar rate of approximately 0.1%. Certain factors may increase the risk of seizure; therefore, prior to the prescription of bupropion, patients should be screened for the presence of medical comorbidities, clinical situations, or concomitant medications that may lower seizure threshold.
From A Review of the Neuropharmacology of Bupropion, a Dual Norepinephrine and Dopamine Reuptake Inhibitor by Stahl et. al., 2004:
An often-debated issue is the incidence of seizure associated with antidepressant therapy. Most antidepressant clinical trials report that the seizure incidence ranges from 0.1% to 0.3% for the newer-generation antidepressants and up to 1.1% for the TCAs. The spontaneous seizure rate reported in the general population is approximately 0.1%. For bupropion, the incidence of seizure reported in the product information for the older, immediate-release formulation (Wellbutrin) is 0.4% at doses up to 450 mg/day, and for Wellbutrin SR and Zyban (also a sustained-release formulation), 0.1% for doses up to 300 mg/day. In addition, a recently conducted review by the manufacturer of its clinical trials database for the sustained-release formulation of bupropion (N = 15,213) showed an overall seizure incidence of 0.07% at doses up to 400 mg/day. The mechanisms by which antidepressants may lower the seizure threshold are largely unknown.
From the FDA:
Dose: At doses of WELLBUTRIN SR up to a dose of 300 mg/day, the incidence of seizure is approximately 0.1% (1/1,000) and increases to approximately 0.4% (4/1,000) at the maximum recommended dose of 400 mg/day.
Data for the immediate-release formulation of bupropion revealed a seizure incidence of approximately 0.4% (i.e., 13 of 3,200 patients followed prospectively) in patients treated at doses in a range of 300 to 450 mg/day. The 450-mg/day upper limit of this dose range is close to the currently recommended maximum dose of 400 mg/day for WELLBUTRIN SR Tablets. This seizure incidence (0.4%) may exceed that of other marketed antidepressants and WELLBUTRIN SR Tablets up to 300 mg/day by as much as 4-fold. This relative risk is only an approximate estimate because no direct comparative studies have been conducted.
Additional data accumulated for the immediate-release formulation of bupropion suggested that the estimated seizure incidence increases almost tenfold between 450 and 600 mg/day, which is twice the usual adult dose and one and one-half the maximum recommended daily dose (400 mg) of WELLBUTRIN SR Tablets. This disproportionate increase in seizure incidence with dose incrementation calls for caution in dosing.
Data for WELLBUTRIN SR Tablets revealed a seizure incidence of approximately 0.1% (i.e., 3 of 3,100 patients followed prospectively) in patients treated at doses in a range of 100 to 300 mg/day. It is not possible to know if the lower seizure incidence observed in this study involving the sustained-release formulation of bupropion resulted from the different formulation or the lower dose used. However, as noted above, the immediate-release and sustained-release formulations are bioequivalent with regard to both rate and extent of absorption during steady state (the most pertinent condition to estimating seizure incidence), since most observed seizures occur under steady-state conditions.
Patient factors: Predisposing factors that may increase the risk of seizure with bupropion use include history of head trauma or prior seizure, central nervous system (CNS) tumor, the presence of severe hepatic cirrhosis, and concomitant medications that lower seizure threshold.
Clinical situations: Circumstances associated with an increased seizure risk include, among others, excessive use of alcohol or sedatives (including benzodiazepines); addiction to opiates, cocaine, or stimulants; use of over-the-counter stimulants and anorectics; and diabetes treated with oral hypoglycemics or insulin.
Concomitant medications: Many medications (e.g., antipsychotics, antidepressants, theophylline, systemic steroids) are known to lower seizure threshold.
Recommendations for Reducing the Risk of Seizure: Retrospective analysis of clinical experience gained during the development of bupropion suggests that the risk of seizure may be minimized if
the total daily dose of WELLBUTRIN SR Tablets does not exceed 400 mg,
the daily dose is administered twice daily, and
the rate of incrementation of dose is gradual.
No single dose should exceed 200 mg to avoid high peak concentrations of bupropion and/or its metabolites.
Footnotes
-
Amotivation and anhedonia and among the negative symptoms of schizophrenia ↩
-
From the linked paper:
When overwhelmed by strong emotions, including anxiety and boredom, some people with ASD may exhibit repetitive “stimming” behavior such pacing, flapping or verbally repeating a certain word or phrase.
-
And strictly speaking any psychiatric use of it is off-label: the only licensed used for Bupropion in Australia is smoking cessation. ↩
-
Software projects are only ever asymptotically finished, but I consider that by the time I wrote that blogpost it was at least in a state where I could show it off to others. ↩